
Introduction
To date, Given the fact that minority patients tend to have less positive health outcomes compared to majority patients (Ashton et al., 2003; Collins et al., 2002; Cooper-Patrick et al., 1999) and that reducing health inequalities is a global imperative (Hosseinpoor, Bergen, & Schlotheuber, 2015; World Health Organization, 2005), the establishment of a more diverse physician workforce can be deemed a pragmatic policy implication for public health intervention efforts (Arendt & Karadas, 2019). In fact, ethnic concordance in patient-physician communicationŌĆöwhere the patient and physician are members of the same ethnic minority groupŌĆöcan beneficially contribute to positive outcomes in minority patients as indicated by non-experimental (Cooper et al., 2003; Saha, Komaromy, Koepsell, & Bindman, 1999; Shin et al., 2005) and experimental evidence (Arendt & Karadas, 2019). Indeed, there is evidence that minority patients in ethnic-concordant patient-physician communication tend to be more likely to use the required health services, show increased continuance in healthcare, are less likely to postpone or delay seeking healthcare, and have more satisfying and participatory office visits (Alegr├Ła et al., 2013; LaVeist & Nuru-Jeter, 2002; Saha, Taggart, Komaromy, & Bindman, 2000).
The establishment of a more diverse physician workforce can thus be deemed to be a valuable public health intervention. Of note, the test of possible unintended effects of (public health) interventions is of utmost importance (Arendt, Hauck, Mayr, & Negwer, 2019). Importantly, we do not know whether there are undesired effects in majority patients based on prejudiced responses. In fact, majority patients might show less positive outcomes when interacting with a minority physician based on their prejudice. Prejudiced responses might elicit an impact in majority patients with outcomes in an undesired direction. The present study contributes to this line of research by testing whether majority patients show less positive outcomes when interacting with a minority physician based on their prejudiced antipathy toward minorities.
Literature Review
Possible Undesired Effects: Prejudiced Responses
A social-cognition account (Arendt, 2013; Greenwald et al., 2002) can be used as the theoretical framework to explain prejudiced responses in majority patients. There are two key components of intergroup bias relevant for physician-patient communication: affect and cognition (Amodio & Devine, 2006; Greenwald et al., 2002). Stereotypes can be conceptualized as cognitive associations that consist of a concept representing a social category such as ŌĆ£minority physiciansŌĆØ and an attribute such as ŌĆ£incompetent;ŌĆØ conversely, prejudice refers to negative affective responses toward members of social categories such as minority physicians. Importantly, stereotypes and prejudice refer to cognitive and affective mental associations that individuals believe characterize an entire social category. Thus, the use of stereotypes and prejudice can keep individuals (e.g., majority patients) from processing new information about each unique individual (e.g., minority physician) because some group-based generalizations are already present (see Arendt, 2013). From an information-processing perspective, stereotypes and prejudice can thus offer efficient shortcuts (see Fiske & Taylor, 2013). Note that the term efficient does not mean accurate.
Once formed, cognitive and affective memory traces mentally associated to a social category can be re-activated (i.e., primed) by exposure to an individual member of a social category (e.g., an individual physician encountered in a medical consultation). This can influence subsequent perceptions of this individual. As perceptions of a physician can be related to both key components of intergroup bias (i.e., cognition and affect), we use ŌĆ£prejudiced responseŌĆØ as a general term to refer to both components.
Previous research has shown that there are racial/ethnic health disparities in health care (LaVeist, 2002). Although the full set of underlying mechanisms are not entirely known, research has revealed that patient-physician communication has been noted as one path of influence that may influence patientsŌĆÖ perceptions of finding common ground with their physicians and with better health outcomes (Johnson, Roter, Powe, & Cooper, 2004; Smedley, Stith, & Nelson, 2002). In fact, ethnic concordance between patients and physicians may improve health outcomes by (1) reducing physiciansŌĆÖ discriminatory behavior based on ethnic bias (bias hypothesis); (2) reducing patientsŌĆÖ stereotypic ingroup preferences (preference hypothesis); and (3) reducing problems related to communication per se (communication hypothesis) (Ashton et al., 2003; Strumpf, 2011).
Importantly, previous research has often relied on race or ethnicity to define the terms ŌĆ£minority patientŌĆØ and ŌĆ£majority patientŌĆØ when investigating intergroup bias in patient-physician communication (e.g., Johnson et al., 2004). However, it is important to note that there is a longstanding controversy and there is no consensus on appropriate terms in the study of the health of minority groups (Bhopal, 2003). In Germany, the term ŌĆ£raceŌĆØ is generally perceived to be problematic due to Germany's Nazi past. The term ethnicity generally emphasizes a mix of factors including language, religion, ancestry, or nationality (see Bhopal, 2003). Consistent with this literature, we focused on prejudice based on the basis of ethnic origin.
The Present Study
Unfortunately, the test of possible unintended effects of (public health) interventions in the health communication domain has not received the attention it deserves and there are calls for a stronger focus on testing such effects (Arendt, Hauck, Mayr, & Negwer, 2019). Undesired unintended effects may show up when majority patientsŌĆÖ prejudice toward minorities may (1) decrease favorable beliefs toward the physician such as sympathy and perceived competence; (2) increase reactance-related outcomes such as perceived manipulation intent and anger toward the physician; and (3) decrease knowledge transfer of the information provided by the physician. Stated formally, there are three research questions related to unintended effects:
RQ1: Does a minority physician (relative to a majority physician) decrease favorable beliefs toward the physician in majority patients?
RQ2: Does a minority physician (relative to a majority physician) increase reactance-related outcomes in majority patients?
RQ3: Does a minority physician (relative to a majority physician) decrease knowledge transfer in majority patients?
Outcomes are all central concepts that have been identified as important by previous research on physician-patient communication (Hall & Roter, 2012) and were also used in a previous experimental study showing the beneficial effects of ethnic concordance in minority patients (Arendt & Karadas, 2019). In this previous study, ethnic concordance improved beliefs in the physician, reduced reactance-related outcomes, and improved knowledge transfer in minority patients. The present study utilized a similar methodology with the same outcomes but tested the effects of ethnic concordance in a majority patient sample. We aim to determine if prejudiced responses occur as an unintended effect in majority patients.
Method
We used a web-based experiment with two conditions to test whether a minority physician elicits undesired unintended effects in majority patients. Individuals living in Germany and self-rated as German (i.e., ŌĆ£majority patientsŌĆØ) were randomly assigned to a hypothetical medical consultation that was led either by a ŌĆ£German majority physicianŌĆØ or by a ŌĆ£Turkish minority physician.ŌĆØ The physician talked about unhealthy diets, tobacco smoking, and physical inactivity; that is, lifestyle factors associated with chronic non-communicable diseases. Using equivalence testing, we tested whether it mattered if majority patients interacted with a minority or a majority physician in the hypothetical medical consultation. Substantial differences between both conditions would indicate unintended effects. Importantly, the physician in both conditions talked about the same kinds of information and provided the same prevention-related recommendations. Only the (stereotypic) name of the physician, which we used for the experimental manipulation, differed between both conditions. After being exposed to the medical consultation, we measured beliefs toward the physician, reactance-related outcomes, and knowledge transfer. In an additional analysis outline below, we also measured the impact of a set of third variables. Finally, the participants were debriefed.
Participants
Individuals were enrolled via a commercial market research company. A total of 305 individuals fulfilled the inclusion criteria and participated in the study after giving their informed consent. The sample ranged in age from 19 to 78 years (M = 50.23, SD = 14.41). Of the participants, 51.8% were male. Of the participants, 41.3% had no high school diploma and 58.7% had a high school diploma (ŌĆ£AbiturŌĆØ). A total of 20% of the sample had a university degree. Furthermore, 100% of the sample indicated that they had German citizenship.
Experimental Manipulation
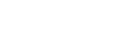
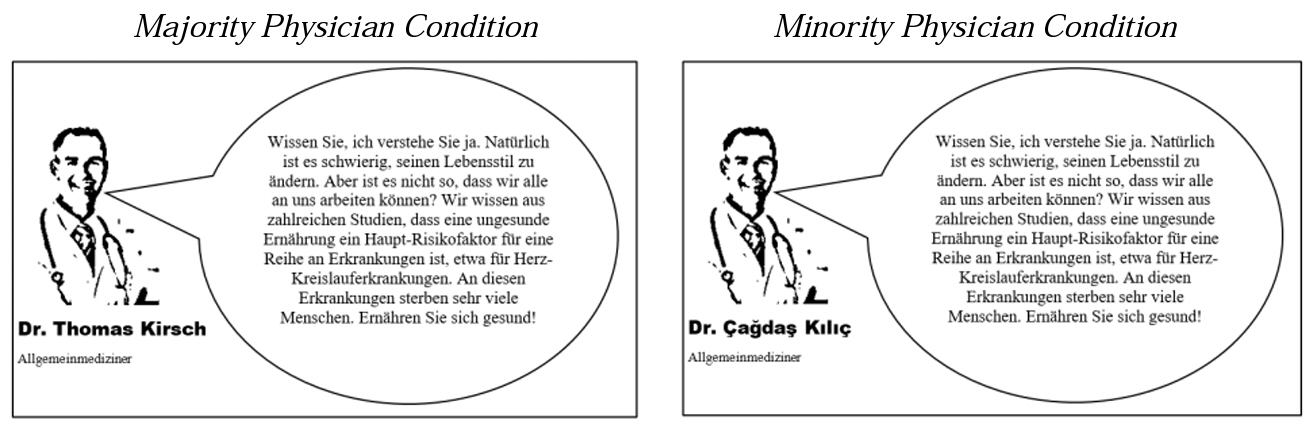
A one-factorial design with two experimental conditions was utilized. Within the ŌĆ£hypothetical medical consultation,ŌĆØ a physician talked about lifestyle factors associated with chronic non-communicable diseases (see Arendt & Karadas, 2019). We used three pictures on three consecutive survey pages, each showing a black and white picture of a physician. The picture only presented the contours of the person and did not provide any reference to their ethnic background. The picture was the same in both conditions. On each of these pictures, we inserted a speech bubble. The physician talked about the consequences of tobacco smoking, an unhealthy diet, and physical inactivity. The content of the physicianŌĆÖs talk was identical in both experimental conditions and we relied on reliable scientific facts for the construction of the talk (Egger, Razum, & Rieger, 2018).
ŌĆó Speech Bubble 1 : ŌĆ£You know, I understand you. Of course, it is difficult to change oneŌĆÖs lifestyle. However, isnŌĆÖt it the case that we can all work on this? We know from numerous studies that an unhealthy diet is a major risk factor for a series of diseases, for example, cardiovascular diseases. Many people are dying of these diseases. Eat healthily!ŌĆØ
ŌĆó Speech Bubble 2 : ŌĆ£It is also proven that many people today are physically inactive. Physical inactivity is a major risk factor for numerous serious illnesses, for example, being abnormally overweight (adiposity) or developing diabetes mellitus. I recommend that you should undertake regular physical exercise.ŌĆØ
ŌĆó Speech Bubble 3 : ŌĆ£Furthermore, tobacco smoking is extremely harmful as well. Smoking can lead to respiratory diseases and malignant tumors. For example, cigarette smoking substantially increases the risk of dying from lung cancer. If you are a smoker, quit! Studies also show that passive smoking has serious health consequences.ŌĆØ
Participants allocated to the minority physician condition (n = 151) were dealt with by Dr. ├ća─¤da┼¤ K─▒l─▒├¦, a physician with a Turkish name. We used a Turkish migration background due to the fact that individuals with Turkish migration backgrounds represent the largest minority group in Germany (Statistisches Bundesamt, 2017). For the participants of the present study (i.e., self-rated Germans), this operationalization was intended as a ŌĆ£minority physician.ŌĆØ Participants allocated to the majority physician condition (n = 154) met Dr. Thomas Kirsch. This name has similar pronunciation to the ŌĆ£TurkishŌĆØ physicianŌĆÖs name but is German in origin. Figure 1 provides an example.
Outcomes
After participating in the hypothetical medical consultation, we measured beliefs toward the physician, reactance-related outcomes, and knowledge transfer. These scales were derived from previous research (Arendt & Karadas, 2019). All items were measured on a 7-point scale (1-7) and item wordings and internal consistency measures can be found in Table 1. Furthermore, we asked participants to indicate whether the nationality of the physician in the hypothetical medical consultation influenced their perceptions of the physician and the content of his talk (Yes, No). For the manipulation check, we asked whether participants thought that the physician was a German doctor, a Turkish doctor, or if they did not remember, the response was I donŌĆÖt remember.
Statistical Analysis
The goal of the present study was to test for possible unintended effects in majority patients. Stated differently, we wanted to show that there are no substantial unintended effects in majority patients. Thus, we wanted to demonstrate equivalence (rather than a difference) between the majority physician condition and the minority physician condition. Therefore, we relied on equivalence tests (Weber & Poporova, 2012). Equivalence tests originated in bioequivalence research, especially in studies that aimed to show that new generic drugs were bioequivalent. In contrast to standard nil-null hypothesis significance testing, equivalence tests are designed to provide evidence for a null hypothesis (ŌĆ£there is no differenceŌĆØ). Importantly, researchers have to define a minimum substantial effect. We specified a minimum substantial effect of ╬ö = 0.30ŌĆöa medium-sized effect according to Cohen (1988). Note that a significant peq value in equivalence testing means that there are no substantial differences (i.e., both groups can be deemed equivalent), which is indicative of no substantial unintended effects. Equivalence tests provide stronger statistical evidence for a lack of undesired unintended effects from an intervention than standard nil-null hypothesis significance testing does (see Weber & Poporova, 2012).
Ethical Approval
The Department of Communication at the University of Vienna, Austria, did not require IRB approval at the time of data collection for conducting and publishing empirical communication research involving non-clinical participants aged over 18 years. Taking part in the survey was voluntary. Participants could refuse to take part or withdraw from the study at any time. Finally, participants were debriefed.
Results
Manipulation Check
We asked participants whether they thought that the physician encountered in the medical consultation situation was a German doctor, a Turkish doctor, or whether they did not remember. A 2 (experimental condition: majority or minority physician) ├Ś 3 (manipulation check perception measure: German physician, Turkish physician, I donŌĆÖt know) cross-tab analysis provides supporting evidence for a successful manipulation, Žć2(2) = 137.60, CramerŌĆÖs V = .67, p < .001. The majority within the majority physician condition (n = 117) remembered consulting with a German doctor compared to a minority (n = 3) remembering having dealt with a Turkish doctor. A similar pattern emerged in the minority physician condition (German doctor: n = 34, Turkish doctor: n = 97). The remaining participants indicated that they did not remember the doctorŌĆÖs nationality. The manipulation was thus successful.
Research Questions: Testing for Unintended Effects
We wanted to determine whether a minority physician could elicit worse outcomes related to beliefs toward the physician (RQ1), reactance-related outcomes (RQ2), and knowledge transfer (RQ3) in majority patients. We found that the majority physician group (M = 4.75, SD = 1.40) and the minority physician group (M = 4.68, SD = 1.45) showed similar beliefs toward the physician, M╬ö = ŌłÆ0.06, 95% CI [ŌłÆ0.38, 0.26]. Similarly, reactance-related outcomes also showed similar means when comparing the majority physician group (M = 2.70, SD = 1.66) and the minority physician group (M = 2.55, SD = 1.54), M╬ö = ŌłÆ0.15, 95% CI [ŌłÆ0.51, 0.21]. The same general pattern could be observed for knowledge transfer between the majority physician group (M = 6.03, SD = 1.09) and the minority physician group (M = 6.06, SD = 1.17), M╬ö = 0.02, 95% CI [ŌłÆ0.23, 0.28]. Note, the confidence intervals include zero, indicating the absence of a substantial effect from the experimental treatment.
Equivalence testing formally supports this interpretation: The minority physician group can be deemed as equivalent to the majority physician group in terms of beliefs toward the physician, t(303) = 0.37, ╬ö = 0.30, peq < 0.001 (two-tailed), reactance-related outcomes, t(303) = 0.81, ╬ö = 0.30, peq < 0.001 (two-tailed), and knowledge, t(303) = ŌłÆ0.16, ╬ö = 0.30, peq < 0.001 (two-tailed). Hence, when using a medium effect size according to Cohen (1988), all three tests for equivalence were significant. Taken together, there were no substantial across-the-board unintended effects in majority patients when interacting with a minority physician.
Discussion
Ethnic concordance in patient-physician communication can beneficially contribute to positive outcomes in minority patients, as previous research has shown. Research has yet to show that there are no substantial undesired effects in majority patients. In fact, majority patients might show less positive health outcomes when interacting with a minority physician based on their prejudiced antipathy toward minorities. However, we found no substantial across-the-board unintended effects related to beliefs toward the physician, reactance-related outcomes, and prevention-related knowledge transfer when interacting with a majority or a minority physician. This clearly supports the ongoing calls for a more diverse physician workforce. Increasing ethnic diversity among physicians is one of the most direct strategies to improve healthcare experiences for minority patients (Cooper et al., 2003). The findings of the present study are consistent with this claim: Although a previous study provided evidence for improved health outcomes in minority patients when interacting with a minority physician using the same methodology as in the present study (Arendt & Karadas, 2019), the present study showed that a minority physician did not elicit across-the-board unintended effects in majority patients. On a general level, it is important to note that unintended effects have to be focused on more in health communication scholarship (Arendt et al., 2019). In fact, we should not only strive to show that interventions elicit desired effects but we should also seek to determine any possible undesired effects.
This study has a number of limitations. First, we used a hypothetical medical consultation to measure the impact of the minority or majority group status of the physician. This experimental strategy has limitations in terms of external validity. However, a hypothetical medical consultation allows for the controlled experimental manipulation of ethnic concordance and thus allows for more confident causal claims to be made. Therefore, we mainly focused on high internal validity. As we outlined above, internal validity has often been limited in previous (largely non-experimental) studies on ethnic concordance. Second, we used self-report measures to assess beliefs regarding the physician, reactance-related outcomes, and knowledge transfer. Importantly, a self-report measure cannot assess whether individuals actually changed their prevention-related behaviors after being exposed to the hypothetical medical consultation (i.e., whether smokers reduced or quit smoking, exercised more, or ate more healthily). Third, we used the physicianŌĆÖs name for the experimental manipulation of ŌĆ£minority physicianŌĆØ and ŌĆ£majority physicianŌĆØ (i.e., Dr. ├ća─¤da┼¤ K─▒l─▒├¦ vs. Dr. Thomas Kirsch). Even though this strategy worked well in the present study (successful manipulation check), it is important to note that ethnicity is a broad concept that includes many variables (see above).
Despite these limitations, the present study emphasizes the importance of a diverse physician workforce. There was no evidence for unintended effects in majority patients, thus there is support for the idea of striving for the establishment of a more diverse physician workforce. Although the present study utilized a web-based experiment in which individuals were randomly assigned to a hypothetical medical consultation (which aimed at simulating patient-physician communication in interpersonal settings), the findings have also implications for other domains in the context of new media environments such as doctors giving online advice on health topics or physician-rating websites. Future studies should investigate the role of ethnic concordance in this domain.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print



